Concern 1: Vaccines contain immoral and illicit biological components such as cells from human fetuses.
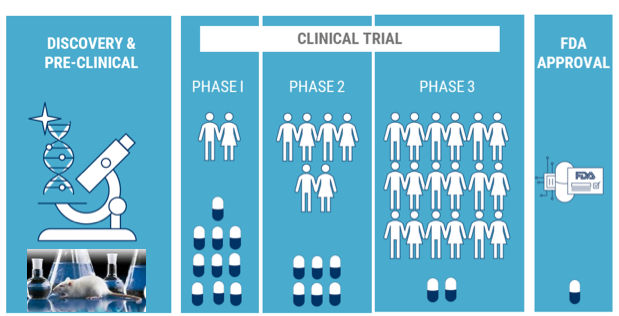
Although vaccines represent an incredible medical breakthrough, they have raised concerns in some quarters: Should devotees, who are firmly opposed to abortion, refuse to use vaccines that are developed using cell lines derived from the tissue of aborted fetuses? Some anti-abortion ethicists have claimed that several vaccines which are approved or are under development are unethical because of their connection to abortion For devotees to address questions about such vaccines we believe it is important to know the facts fully in order to make a fully informed choice. To understand the subject, let us ask some questions- Q. 1. Are the fetal ‘cell lines’ the same as the fetal ‘tissue’? The answer is NO. Fetal cell lines are cells that grow in a laboratory. Although it is true that these cells were initially derived from the tissue of an aborted fetus (after legal and elective termination of two pregnancies in 1972 in Netherlands), they have since multiplied into many new cells over the past four or five decades, creating fetal cell lines. Thus, the current fetal cell line, popularly known as HEK 293 (Human Embryonic Kidney) is thousands of generations removed from the original fetal tissue. Q. 2. Do we need to abort fetuses repeatedly to harvest these cell lines? The answer is NO. Once these cells were harvested in 1972 from the fetal tissues, they were genetically modified in such a way that they continue to divide and reproduce themselves indefinitely.These cells are called as immortal cells and such cell lines thus do not require ongoing abortions or additional demand for new fetal tissue. Even though no additional fetal cells need to be harvested, the topic of using these cells remains controversial because of their original source. Despite the issues concerning their origin, these cell lines continue to offer an easy, inexpensive and stable platform for researchers to test and develop efficacy of drugs/vaccines. Q. 3. Why are human fetal cells the choice of the researchers and why not any other cells (from animal origin)? a) Viruses need a host to grow/replicate b) Viruses replicate better in cells derived from humans than from animals (because humans are their natural host). c) Naturally all cells die after dividing a certain number of times and this number is known as the Hayflick limit. For most cell lines, it is around 50 divisions; however, because fetal cells have not divided as many times as other cell types, they can be cultured in a laboratory setting for a longer period of time. Q. 5. Would the vaccine produced or tested using these cells contain traces of these cells? The answer is NO. Although fetal cells are used to either test the efficacy of vaccines (during the study phase) or grow vaccine viruses in large scale (during production or manufacturing phase), the final product does not contain these cells. Why? Concern 2: Vaccines contain toxic ingredients that cause adverse reactions including autism and other diseases in children and adults. 1. Mercury Thimerosal (USA)/Thimersol (UK) is a mercury-based preservative that has been used in vaccine formulation. Thimerosal is added to the vaccine vials that contain more than one dose (multi-dose vials) to prevent growth of germs, like bacteria and fungi (a contaminated vaccine can be deadly if injected). Vaccine vials have a potential to be contaminated each time a medical practitioner introduces a fresh syringe in the glass vial before administration. Mercury is a naturally occurring trace element found in the earth’s crust, air, soil, and water. There are two types of mercury to which people may be exposed-methylmercury and ethylmercury. These two forms of mercury are totally different, and their exposure have entirely different consequences. While methylmercury is found in certain kinds of fish and at high exposure levels can be neurotoxic; Thimerosal contains ethylmercury, which does not stay in the body for a long time and is cleared from the human body more quickly than methylmercury and is therefore less likely to cause any harm. At concentrations found in vaccines, 0.01% (1 part in 10,000), Thimerosal meets the requirements for a preservative as set forth by the United States Pharmacopeia (2004). For comparison, this is roughly the same amount of elemental mercury contained in a 3 ounce can of tuna fish (of course we don’t eat this, but this is just to give an idea of the safety). Although, data from many studies provide evidence of no harm caused by the low doses of thimerosal in vaccines, except for minor reactions like redness and swelling at the injection site, in July 1999, the Public Health Service (PHS) agencies, the American Academy of Pediatrics (AAP), and vaccine manufacturers agreed that thimerosal should be reduced or eliminated in vaccines as a precautionary measure. Therefore, it was taken out of childhood vaccines in the USA in 2001 and was removed from UK vaccines between 2003 and 2005. Today, no childhood vaccine used in the USA contains Thimerosal, except the Influenza (flu) vaccine. However, Influenza vaccines currently available are also in both thimerosal-containing (multi-dose vials) and thimerosal-free (single dose vials) versions. To circumvent the need of adding preservatives, all childhood vaccines are now put as single-dose vials which are used and thrown after a single use. Further, many robust and peer-reviewed research studies have concluded that Thimerosal in vaccines does not contribute to the development of autism (National Academy of Medicine, 2004). A 2014 Australian study of over a million children found no evidence of a link between thimerosal in vaccines and autism. It is also worthwhile noting the fact that, even after thimerosal was removed from almost all childhood vaccines, autism rates continued to increase, which is the opposite of what would be expected if thimerosal caused autism. 2. Aluminum Some vaccines contain aluminum salts, such as aluminum hydroxide, aluminum phosphate or potassium aluminum sulphate, which are used as adjuvants. Adjuvants are substances that are often added to the vaccines to strengthen and lengthen the immune response to the vaccine. Aluminum salts appear to slow down the release of the active ingredient from the vaccine once it is injected and stimulate the immune system better to respond to the vaccine. They also absorb protein well and prevent the sticking of the proteins (present in the vaccine) to the walls of a vial during storage. Aluminum is the most common metal in the earth’s crust, and we are exposed to it all the time. We get aluminum in our body from other common sources as well, which include drinking water, breast milk and infant formula, or use of health products such as antacids, buffered aspirin, and antiperspirants/deodorants. Aluminum salts are used as food additives (for example in bread and cakes) and aluminum is widely used in food packaging. Aluminum is not retained in the body. Any aluminum absorbed from food or other sources is gradually eliminated through the kidneys. Experts have not found any convincing evidence that exposure to everyday levels of aluminum in any form increases the risks of Alzheimer’s disease, genetic damage, or cancer. A study from 2011 modeled the impact of aluminum from diet and vaccines in infants and concluded that the total amount of aluminum absorbed from both sources was likely to be less than the weekly safe intake level. A study from 2002 drew similar conclusions. Although vaccines that contain aluminum are associated with more redness and hardness (granuloma) at the injection site than other vaccines, granulomas are not life-threatening and disappear with time. 3. Formaldehyde Several other components like formaldehyde/formalin could be existing in trace amounts in vaccines. To generate inactivated vaccines, formaldehyde is used to kill viruses or inactivate toxins during the manufacturing process. However, the amount of formaldehyde present in some vaccines is so small compared to the concentration that occurs naturally in the body that it does not pose a safety concern. 4. Sorbitol and other stabilizers like gelatin Sorbitol is produced naturally in the human body and is also found in fruits and berries. It is commonly used as a sweetener in foods and drinks. In vaccines, it is used in small quantities as a stabilizer. Sorbitol is usually harmless, but people with an allergy to sorbitol, or with rare inherited problems of fructose intolerance, should not receive vaccines containing sorbitol. Other commonly used stabilizers that are used in vaccines in very small quantities are: sugar (sucrose), milk sugar (lactose), urea (harmless organic compound in our body), glycerol (non-toxic substance used as a food additive) Gelatin derived from pigs is used in some live vaccines as a stabilizer to protect live viruses against the effects of temperature. Gelatin in vaccines is highly purified and hydrolyzed (broken down by water), so it is different from the natural gelatin used in foods. Gelatin is used in some vaccines licensed in UK, Nasal flu vaccine (Fluenz), MMR (MMRVaxPro), Shingles (Zostavax), Chickenpox (Varivax); and in USA, live attenuated influenza (FluMist), MMR II®, MMR-Varicella (ProQuad®), Rabies (Rabavert®), Typhoid oral (Vivotif®). In 1993, Kelso and co-workers reported the case of a 17-year-old girl in California who developed a severe allergic reaction (hives, low blood pressure, runny nose, and lightheadedness) within five minutes of receiving an MMR (measles, mumps and rubella) vaccine. Her symptoms resolved after treatment with epinephrine. Describing the event later, the girl stated that it was “kind of like what happens when I eat Jell-O®.” Subsequent testing found that the only component of the vaccine to which this girl was allergic was gelatin. Studies in Japan confirmed the findings of Kelso and colleagues that severe allergic reactions to MMR vaccine were associated with the presence of antibodies in the blood directed against gelatin. Although the incidence of anaphylaxis to gelatin is extremely low (about 1 case per 2 million doses), gelatin is the most common identifiable cause of severe allergic reactions to vaccines. 5. Eggs Besides growing or testing viruses in fetal cells (HEK293), some vaccines, like MMR and some flu vaccines, are grown in eggs, which help manufacturers to grow enough of the virus or bacteria needed to make the vaccine in bulk. Growing viruses in eggs is the oldest way of making flu vaccines. Scientists inject a live virus into an egg, let the virus replicate, collect the virus, harvest and purify them, and then kill the virus. This implies that some egg proteins (like ovalbumin) are present in the final vaccine product. While not all manufacturers disclose the amount of ovalbumin in their vaccines, those that did from 2011-2012 through 2014-2015 reported maximum amounts of ≤1 µg/0.5 mL dose for flu shots and 0.24 µg/0.2 mL dose for the nasal spray vaccine. Based on scientific evidence, the American Academy of Pediatrics (AAP) states that the MMR vaccine can be safely given to all patients with egg allergies, including patients with a history of severe, generalized anaphylactic reactions to eggs. AAP also states that “children with egg allergy can receive influenza vaccine with no additional precautions than those considered for any vaccine.” Concerns about COVID-19 Vaccines in particular Concern 1: Do the COVID-19 vaccines contain aborted fetal cells? The answer is NO. COVID-19 vaccines do not contain any aborted fetal cells. Neither Pfizer/BioNtech nor Moderna or AstraZeneca (Covishield) vaccines used fetal cell lines for the development or production of the vaccine. However, scientists did use the immortalized fetal cell line (HEK 293), ONLY to ensure that the vaccines work (efficacy studies). Since no fetal cell lines were used to manufacture or produce the vaccine, they are not inside the final injection dose we will receive. Concern 2: Oxford/AstraZeneca viral vector vaccine contains components from chimpanzees? Q.1. How does Oxford/AstraZeneca Vaccine work? Oxford/Astrazeneca vaccine uses an engineered virus called adenovirus, which is designed to transport/shuttle a gene from COVID-19 into our bodies where our cells will read it and make coronavirus spike protein. As with all vaccines, the idea is to trick our body into thinking that it has been infected. Presence of these self-made spike proteins would stimulate our immune system to make antibodies against the spike protein of coronavirus so that in future when we are exposed to the live virus, the antibodies will detect and terminate the virus before it can wreak havoc. Scientists have modified this adenovirus in a way that it can enter the human cells but can’t replicate inside our body or cause infection. This is done by replacing a portion (20%) of the genome of this adenovirus and replacing it with the information to make the spike protein of COVID-19. After the vaccine is injected into a person’s arm, the adenovirus enters into the cells by latching their proteins onto the cell surface (as shown in the Figure). The cell engulfs the virus in a bubble and pulls it inside. Once inside, the adenovirus escapes from the bubble and travels to the nucleus, where the cell’s DNA resides. The adenovirus pushes its DNA into the nucleus (it doesn’t affect the cell’s DNA). The adenovirus is engineered so it can’t make copies of itself, but the gene for the coronavirus spike protein can be read by the cell and copied into a molecule called messenger RNA, or mRNA. This mRNA travels to the cytoplasm where it generates copies of the Covid-19 spike protein. This protein will be recognized as foreign by our body and stimulate the immune system to make antibodies against it. When the vaccinated person is confronted with the Covid-19 virus, these pre-existing antibodies can latch onto the coronavirus spikes and prevent infection by blocking the spikes from attaching to the cells. Q.2. Does Oxford/AstraZeneca vaccine have components from Chimpanzees? The answer is NO. Adenoviruses are common viruses that typically cause cold or flu-like symptoms. The Oxford-AstraZeneca team used a virus (that is known to cause flu in chimpanzees) to deliver the information (DNA) coding for the COVID-19 spike protein. This virus was used only as a vehicle to deliver the genetic information. It was not isolated from chimpanzees nor does it contain any biological components from Chimps. Q.3. How is the Oxford/AstraZeneca virus different from Pfizer/BioNtech and Moderna vaccines? The Oxford/AstraZeneca vaccine uses a virus to release double-stranded DNA coding for the spike protein. However, the Pfizer-BioNTech and Moderna vaccines, use a lipid nanoparticle to deliver single stranded mRNA (what is mRNA is discussed in the Vaccine article_Part 1) coding for the spike protein. Frequently Asked Questions (FAQs) about COVID-19 vaccines FAQ1: What are the different vaccines approved in India? Are they safe and effective? India is currently relying on two major vaccines: A. Covaxin: India‘s indigenous (home grown) COVID-19 inactivated vaccine by Bharat Biotech (Hyderabad) is developed in collaboration with the Indian Council of Medical Research (ICMR) and National Institute of Virology (NIV). To create Covaxin, researchers at NIV isolated coronaviruses in large stocks and then doused them with a chemical called beta-propiolactone. The inactivated coronaviruses can no longer replicate but their proteins, including spike, remained intact. (refer to the appendix for more information on types of vaccines to learn more about Inactivated vaccines). Q.1. How does it work and what does it contain? Even though Covaxin uses the whole virus, since the virus is inactivated, it can be injected into the arm without causing COVID-19. Once inside the body, the inactivated virus triggers the immune system to generate antibodies. Once vaccinated with Covaxin, the immune system is expected to respond to a future infection of live COVID-19. Further, Covaxin uses aluminum based adjuvant “Alhydroxiquim-II” to boost immune response and longer-lasting immunity. Q.2. Is it safe and are there any side effects reported for this vaccine? YES. After successful completion of the interim analysis from the Phase 1 & 2 clinical trials, Bharat Biotech received approval for Phase 3 clinical trials in 26,000 participants in over 25 centers across India. Recently, one death was reported in a phase 3 trial volunteer (from Bhopal), 9 days after the first jab. But the cause of death was not linked to the vaccine or placebo, rather cardiac respiratory failure as a result of suspected poisoning. On January 21st, 2021, the data for Phase 1 clinical trial was published in a reputed medical journal, “Lancet”. The vaccine was tested on 375 volunteers between the ages of 18 and 55 years. It was found to be well-tolerated in all groups with mild side effects like fatigue, headache, fever and pain at the injection site. Despite these favorable and optimistic data from trial 1 and lack of Phase 3 data on the complete safety and efficacy of the vaccine, India had authorized this two-dose (4 weeks apart) vaccine regimen for emergency use on January 3rd. However, the manufacturers have provided some information on who should NOT take the vaccination. This includes those with previously reported allergies to any drug/food/vaccines, pregnant/breast-feeding women, those with blood disorders or on blood thinners and immunocompromised patients. Unlike Covaxin, efficacy from phase-3 trials are known for Pfizer, Moderna and AstraZeneca vaccines that people are getting in the developed countries, it is true that people in India have to rely on what is available so far considering the efficacy and interim safety data from the Phase-3 trials of Covaxin are not yet available. B. Covishield: Oxford-AstraZeneca adenoviral vector based vaccine made by the Serum Institute of India. Q.1. How does it work and what does it contain? Already discussed in Questions 1 and 2 under Concern 2. Q.2. Are there any side effects reported for this vaccine? Minimal, not life threatening. Interim data for Oxford/AstraZeneca vaccine from phase 3 trials in adults aged 18 years and older in Britain South Africa and Brazil revealed promising results. In those who received two full doses which are 28 days apart, the vaccine was 62% protective. But it appears to work better when given initially as a half-dose followed by a full dose, with protection then rising to 90%. More than 20,000 volunteers were involved in the trials and half of those were in the UK. There were 175 serious adverse events reported, 84 in the vaccinated individuals and 91 in the control group. The data indicates that three of those were possibly related to the intervention: (a) Inflammation of the spinal cord (transverse myelitis) 14 days after the booster vaccination, (b) hemolytic anemia in the control/non vaccinated recipient, and (c) fever higher than 40°C in a participant still masked to group allocation. Two additional events of transverse myelitis were reported but they were unlikely to be related to the intervention: Q.3. What are the concerns around Covishield vaccine and is it approved for use despite the side effects? The transverse myelitis cases not only resulted in temporary suspension of the trial, but there were also doubts about the data. The biggest questions were, why was there such a large variation in the effectiveness of the vaccine at different doses, and why did a smaller dose appear to produce much better results? Depending on the strength at which the doses were given, the vaccine appeared to be either 90 or 62% effective, with average efficacy around 70% (for comparison, the annual flu shot is usually between 40% and 60% effective, as per the CDC). The regimen that appeared to be 90% effective is based on participants receiving a half dose of the vaccine followed a month later by a full dose; the less effective version involved a pair of full doses. Although it was a lucky mistake, only fewer than 2,800 volunteers got the half-strength initial dose. This is a very small sample size not enough to consider its efficacy for the entire population. Adding to the confusion, AstraZeneca pooled the results from two differently designed clinical trials in Britain and Brazil, which is not a standard practice in reporting the results of drug and vaccine trials. Despite some uncertainty over trial results and dose variation, Britain had authorized the vaccine for emergency use in December, and India had authorized its use on January 3rd. FAQ2: What is the need of different vaccines for different Countries (why not have one vaccine for the whole world)? Are these vaccines affordable and accessible? Among the COVID-19 vaccines furthest along in development or in market, the Oxford/AstraZeneca candidate seems to be the most affordable to low- and middle-income countries considering much of the world’s population currently lives in such settings. Q.1. How is Oxford/AstraZeneca advantageous for the developing countries? Advantages stem from its components which are more stable. Due to the above reasons, the Oxford vaccine doesn’t have to stay frozen. It can also be stored in standard refrigerators, making distribution far easier. The vaccine is expected to last for at least six months when refrigerated at 38-46°F (2-8°C). Hence the Oxford/AstraZeneca vaccine has become a leading contender for the lower-income countries. Q.2. What are the major disadvantages with the Pfizer-BioNTech and Moderna vaccines? Moderna’s vaccine requires long-term storage at minus 20 degrees Celsius (minus 4 degrees Fahrenheit) and is stable for 30 days at refrigerator temperatures between 2 and 8 degrees Celsius (36 to 46 degrees Fahrenheit). Meanwhile, the Pfizer-BioNTech vaccine demands ultra-cold temperatures of minus 70 degrees Celsius (minus 94 degrees Fahrenheit) or lower, with about five days of shelf life at refrigerator temperatures. This is the major distribution hurdle Moderna and Pfizer-BioNTech are working to overcome. FAQ3: Is there a best COVID-19 vaccine I should take if given an option? No definitive answer at this moment. Vaccine trials need to run for several years on a diverse population to get a conclusive understanding on which vaccine is the best. All the vaccines approved so far are ONLY for Emergency Authorization Use (EAU), given the nature of the pandemic. Thus, there is NO “best” vaccine. For all the three vaccines, the side effects are similar, including potential injection site pain (sore arm) and flu-like symptoms, including fever, fatigue, chills, headaches, and muscle pain. Such symptoms are natural and expected post immunization. This is because our immune system is stimulated upon encountering a foreign substance. Thus, development of such symptoms does not necessarily signal that the vaccine is unsafe. FAQ4: If I get vaccinated, do I still need to wear a mask, practice social distancing and continue taking all the precautions? YES. What we must remember at all times is that vaccines aren’t silver bullets, especially as the pandemic rages on. No matter which COVID-19 vaccine becomes available to us first, we should continue being cautious until positive cases, hospitalizations, and deaths are significantly reduced nationwide. And there are two reasons for that: 1) We are not going to be fully protected. In the clinical trials, there were instances where people still contracted COVID-19 after getting the vaccine; this is because the body takes time to develop immunity and also the extent of protection varies with each individual. 2) There is no evidence so far that having had the vaccine will prevent us from getting the virus and also passing it on to others. Vaccines are largely preventing people from developing severe symptoms that need hospitalizations. There is no evidence yet that one dose – or even two – of the existing vaccines will prevent people from getting and giving the virus to others. And we DO KNOW that it’s possible to contract COVID-19 infection even after someone is vaccinated (asymptomatic mild infection). Therefore, although vaccines/drugs are the best prophylactics, we should not let our guards down and continue to follow the additional safety requirements set in place by the CDC and our local Governments like masks, hand-washing, and social distancing. FAQ5: Will I be protected if I only take the first dose and skip the second one (booster dose)? After how many days of vaccination, I can expect to be completely protected and for how long? Do I have to take COVID-19 shot annually? There are several vaccines that do require a booster dose to work. For example, MMR vaccine for infants, Hepatitis B, Shingles and HPV. The available data continue to support the use of two specified doses of each authorized vaccine at specified intervals (priming dose and boosting dose). It is advisable to not think “one is better than none”. We do need both. Q1. How does the booster work and why is it important? When the immune system first encounters a vaccine, it activates two important types of protective cells: Pfizer and BioNTech themselves have urged caution on the grounds that their data ends at day 21, and “there is no data to demonstrate that protection after the first dose is sustained after 21 days“. It’s possible that the protection people seem to have will suddenly drop off after that point. Therefore, the chief executive of Pfizer, Albert Bourla, stated that it would be a “big mistake” to skip the second dose, as it almost doubles the amount of protection conferred. Q2. How effective is a single dose of each of the COVID-19 vaccines? According to Pfizer data published in December 2020, the Pfizer-BioNTech vaccine is roughly 52% effective after the first dose. Further, the protection doesn’t kick in until at least day 12. It is clear from the data that one dose is significantly less protective than two. The latter is 95% effective at preventing the disease after a week. For the Oxford-AstraZeneca vaccine, things are a bit different. In a paper published in January 2021, the authors explain that the vaccine offers protection of 64.1% after at least one standard dose. This compares to 70.4% if you’ve had two full doses, or – oddly – 90% in people who have had one half dose followed by one full dose. For the Moderna vaccine, the data shows that it can provide 80.2% protection after one dose, compared to 95.6% after the second (in people aged 18 to 65 – it’s 86.4% in those over 65). Q3. How long the immunity from these vaccines will last and do we need to take COVID-19 vaccine every year like the flu shot? At this time, no one knows with certainty how long the vaccines may end up protecting us. The trials have not gone long enough to make that determination. More data and more studies are needed. We have to remember that the vaccines have received emergency use authorization (EUA), not full approval. That means that there is still much to learn about the vaccines. Additionally, there are no mRNA vaccines so far in the market, the world is in uncharted territory. There are still many unknowns, such as whether the mRNA vaccines (Pfizer or Moderna) will work just as well in people from different ethnicities, age groups, etc and how long the immunity will last. Regarding the adenoviral based AstraZeneca vaccine, though adenoviruses have been used in cancer vaccines and gene therapy for years, they had only ever been used once before to prevent a viral infection – an Ebola vaccine using this method was approved for use in European Union countries only in July 2020. Since the virus is showing signs of mutations, it might be possible that the vaccines have to be revised each year or alternate years to match with the predominant infecting strain. But it is premature to comment on this precisely. So while the global roll-out of the new vaccines may be exciting, it looks like most of us will have to wait a while longer before normal life can resume. FAQ6: If I have already had COVID-19 and recovered, do I still need a vaccine? The answer is absolutely YES. Getting COVID-19 might offer some natural protection or immunity from re-infection with the virus that causes COVID-19. But it is not clear how long this protection lasts. Also, what degree of immunity one may develop after infection largely depends on a variety of factors such as how severe the first bout of COVID-19 was. Moreover, there have already been confirmed cases of re-infection with the virus. And some cases of re-infection have been more severe than the initial infection. Because re-infection is possible and COVID-19 can cause severe medical complications, it’s recommended that people who have already had COVID-19 get a COVID-19 vaccine. However, a person who had COVID-19 is advised to wait until 90 days after the diagnosis to get a COVID-19 vaccine. Thus, both natural immunity and vaccine-induced immunity are important aspects that experts are still trying to learn for COVID-19 in particular. FAQ7. Are the present-day vaccines effective in protecting us from the rapidly spreading mutant strain of COVID-19, especially those found in Britain (UK), South Africa and Brazil? The emergence of new, and apparently more transmissible coronavirus variants has prompted widespread concern as to whether existing vaccines, including the Pfizer/BioNTech jab, will remain effective? On January 20th, 2021 Pfizer revealed results from an additional study on the efficacy of vaccines to counteract and protect from the UK-COVID-19 mutant strain, also known as B.1.1.7. The B.1.1.7 is a rapidly spreading variant of SARS-CoV-2 initially detected in the U.K. that carries 10 distinct mutations or important changes that changed the structure of the spike protein. Pfizer/BioNtech have investigated the efficacy of their vaccine on the repertoire of mutations found in UK strain. The data showed that the sera of the vaccinated participants had antibodies that could neutralize this pseudovirus containing mutated spike. Thus, it is very unlikely that the mutated UK variant will escape from the protection provided by the present-day Pfizer vaccine. However, the newly found South African (B1.351) and Brazilian variants (P1 and P2) are distinct from the UK strain due to the presence of additional mutations. As of now, whether the Pfizer/BioNTech vaccine will provide protection from the variant viruses that are prevalent in South Africa and Brazil is still a question mark. The current virus landscape is evolving and there is not data as of yet to show that the current vaccines will be ineffective against the newer mutations. It should be also noted that the vaccines can very easily be manipulated in the laboratory to produce more effective versions against any potentially resistant mutations of the virus. FAQ8: What is the spiritual perspective on depending on medicines/vaccinations that are products of biological research and experimentation? Are we severely implicated in karmic reactions? As devotees, we should just have faith in the Lord’s protection and not in mundane science or measures? We cannot deny the fact that scientific research does use animals or animal/human derived components to develop medicines/vaccines etc. Public approval for any drug (as simple as aspirin or paracetamol)/vaccine comes only after receiving a compliance from the relevant national health authority, whose decision is dependent solely on the evaluation of safety and efficacy data generated in the research laboratories using mice, guinea pigs, rabbits and monkeys (called as Pre-clinical trials). Therefore, anyone who wants to completely avoid benefiting from the use of such products would technically have to eschew the use of any medical treatments or biological knowledge developed or updated within the past forty years. Even Ayurveda depends on intense testing on animals. Here is an excerpt from a morning walk with Prabhupada on June 27, 1976 in New Vrindavan: Prabhupāda: Yes. Yes. Āyur Veda. There is a book. Dravya–guṇa. All kinds of herbs, metals, even different kinds of flesh of different animals, they are mentioned. Hundreds of different kinds of animals flesh, how it can be utilized for certain disease, the descriptions are there. Hari–śauri: They use flesh for curing things? Prabhupāda: Hmm? Hari–śauri: They use flesh for curing diseases? Prabhupāda: Yes. Animal-killing is only allowed when it is absolutely necessary, for medicine. Suppose by killing one animal hundreds of lives are saved, so that is allowed. One preparation is chagalaka-ghṛta. It is prepared… A live goat is put into the ghee with other ingredients, and that is a good medicine for tisis(?). Prabhupāda: Tisis(?) Tuberculosis. Overall to summarize, Srila Prabhupada wasn’t neglectful of his own health or the health of his disciples. In fact, Srila Prabhupada always concluded his letters with: “I hope this meets you in good health.” The underlying principle of Prabhupada’s instructions regarding health was “do the needful” for keeping body and soul together in order to serve Krishna. Some of his conversations in the form of letters is provided below for reference: “Regarding your physical malady, you should do whatever is required to treat it properly. Whatever is most practical.” (Srila Prabhupada Letter, May 7, 1975) “One of the symptoms of a devotee is that he is kind, so if our Godbrother becomes ill it is our duty to help him get the proper medicine and treatment so that he can recover.” (Srila Prabhupada Letter, April 5, 1974) Prahalad Maharaja prayers in Srimad Bhagavatam (7.9.19), “My Lord Nṛsiṁhadeva, O Supreme, because of a bodily conception of life, embodied souls neglected and not cared for by You cannot do anything for their betterment. Whatever remedies they accept, although perhaps temporarily beneficial, are certainly impermanent. For example, a father and mother cannot protect their child, a physician and medicine cannot relieve a suffering patient, and a boat on the ocean cannot protect a drowning man”. In the purport to this verse, Prabhupada states that unless one is protected by the mercy of the Lord, no remedial measure can act effectively. One should consequently depend fully on the causeless mercy of the Lord. “BUT as a matter of routine duty one must of course accept other remedial measures”. Thus, taking necessary treatment for curing ailments in no way undermines our faith in Krishna. As devotees, we do understand that Krishna is the ultimate protector. But it is also said, “do your best and leave the rest” A devotee uses everything in the service of the Lord including his body. To underscore this, Lord Chaitanya Mahaprabhu emphatically declared to Sanatan Goswami and Murari Gupta and many of His intimate associates at several instances that this body of theirs is not their own property but it belongs to the Lord. In light of this principle, to protect the lives of devotees and our leaders from terrible diseases like cancer, Alzheimer’s or COVID-19 (in the present context), it is necessary that we resort to therapies or scientific interventions without any hesitation or a second thought. We certainly want to save the lives of devotees and especially the leaders of our movement. Appendix There are 2 main types of vaccines: Live vaccines use a weakened (or attenuated) form of the germ that causes a disease. Live vaccines are derived from “wild,” or disease-causing, viruses or bacteria. These wild viruses or bacteria are attenuated, or weakened, in a laboratory, usually by repeated culturing. For example, the measles virus used as a vaccine today was isolated in 1954 from a child with measles. It took 10 years of repeated culturing to transform the wild virus into an attenuated vaccine virus in the laboratory. A relatively smaller dose of live bacteria or virus is administered to a healthy individual. In the body, these live organisms multiply and grow to an amount that is enough to generate an immune response that would impart protection when actual infection happens. In order to generate an immune response, these weakened germs must replicate (grow) in the vaccinated individual. Although these germs can multiply in the body, they usually do not cause the disease. But since these vaccines contain a small amount of the live virus, sometimes as a result of uncontrolled replication (growth) of the vaccine virus in the body, these LAV might cause disease, which is referred to as an “adverse reaction”. But the form of disease these vaccines cause is usually much milder than the natural disease. Moreover, the incidences of vaccines causing adverse, severe, or fatal reactions are reported in only some people with weakened immunity or underlying health problems or other comorbidities. Such people need to consider risk evaluation before vaccination. According to the CDC, individuals with compromised immune systems, undergoing treatment with certain drugs or on medications, and patients with organ transplant or HIV infection are at high risk. It is noteworthy to mention here that a LAV could theoretically revert to its original pathogenic (disease-causing) form. However, such incidences are rare and were reported only with the live (oral) polio vaccine. A general rule of thumb is that the more similar a vaccine is to the disease-causing pathogen, better is the immune response to the vaccine. Because LAV is virtually identical to a natural infection, the immune system does not differentiate between an infection caused with a weakened vaccine virus or a live wild virus. Therefore, only one dose of the LAV is generally sufficient to provide recipients with a strong and long-lasting immunity. However, for some LAVs like MMR or Varicella, recipients do not respond effectively to the first dose of vaccine and a second booster dose is recommended to provide a high level of immunity in the majority of the population. Inactivated vaccines use the killed version of the germ that causes the disease. Inactivated vaccines are produced by growing the bacterium or virus in a laboratory, then inactivating it with heat and/ or chemicals (usually formalin). Since inactivated vaccines are not alive and cannot replicate, these vaccines cannot cause disease from immunization, even in an immunodeficient or immunocompromised individual. In contrast to the immunization with live vaccines, which closely resemble natural infection, the immune response to an inactivated vaccine is weaker and may diminish with time. As a result, some inactivated vaccines may require periodic supplemental doses to increase, or “boost,” the antibody titers progressively to keep oneself protected. Q1. What is a clinical trial? Clinical trials are research studies performed in people that are aimed at evaluating a medical, surgical, or behavioral intervention. They are the primary way that researchers find out if a new treatment, like a drug or diet or medical device (for example, a pacemaker) is safe and effective in people. Q2. How does a clinical trial begin? Before the U.S. Food and Drug Administration (FDA) approves a clinical trial to begin, scientists perform laboratory tests and studies in animals to test a potential therapy’s safety and efficacy. These preliminary discovery studies are classified under Preclinical trials. If these studies show favorable results, the FDA gives approval for the intervention to be tested in humans. Q3. What are the four phases of a clinical trial? Clinical trials advance through four phases to test a treatment, find the appropriate dosage, and look for side effects. The FDA typically requires Phase I, II, and III trials to be conducted to determine if the intervention (drug/device/diet/vaccine) is safe and effective and can be approved for clinical use. A Phase IV trial for drugs or devices takes place after the FDA approves their use. A device or drug’s effectiveness and safety are monitored in large, diverse populations over a longer timeframe. This is because sometimes, the side effects of a drug/vaccine/device/diet may not It is important for clinical trials to have participants of different ages, sexes, races, and ethnicities. When research involves a group of people who are similar, the findings may not apply to or benefit everyone. When clinical trials include diverse participants, the study results will likely have a much wider applicability. Researchers need the participation of older people in their clinical trials so that scientists can learn more about how the new drugs, therapies, medical devices, surgical procedures, or tests will work for older people. Many older people have special health needs that are different from those of younger people. For example, as people age, their bodies may react differently to drugs. Older adults may need different dosages (or amounts) of a drug to have the right result. Also, some drugs may have different side effects in older people than younger people. Having seniors enrolled in drug or vaccine trials helps researchers get the information they need to develop the right treatment for older people. Bibliography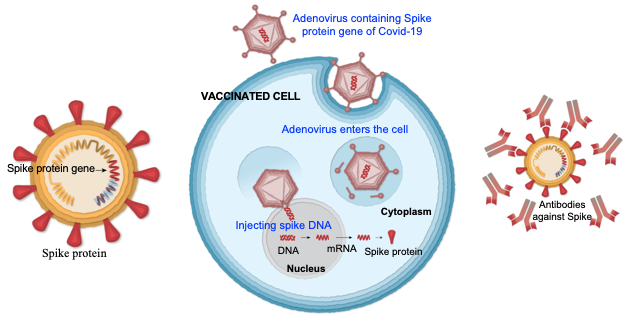
Q4. Why is diversity in participants important in clinical trials?
Addressing the concerns about vaccines in general